SEC conference call between players and medical teams

Just an interesting look at the actual conversations being held behind the scenes.
https://www.washingtonpost.com/sports/2020/08/01/sec-football-players-safety-meeting/
Comments commence!

Same with my golf scorecard.
Colon meme: please stop using me.
I was wondering if someone was going to post this. It was an interesting article. I like your strategy for actually requiring people to read it, if they want to intelligently comment. The article offers quotes to satisfy the ““My advice is you’re going to have to go live your life in this environment“ argument as well as the “We want to play. We want to see football. We want to return to normal as much as possible. But it’s just that with all this uncertainty, all this stuff that’s still circulating in the air, y’all know it kind of leaves some of us still scratching my head. ..” concern.
I meant to note in the OP that the article includes links to various parts of the audio exchanges.
The players that participated were part of a "leadership council," and they seemed much more skeptical than previous reporting on player positions would have you believe. Still, just an interesting direct exchange, and I continue to believe that everything is tentative until campuses are fully populated.
As a player, if you decide not to play, you may give up your place on the team for next year. New guys coming in, coaches looking at those who stayed and put in effort, one year of training and playing experience, lost, etc....But if you play, you risk getting sick. Could be mild and no big deal, or you could be one of those who has lasting effects, or who spreads it to others. There are no right or easy answers for the players. I feel for them and their parents, and what must be a heavy weight to bear.
I'm sorry, but "... But if you play, you risk getting sick. Could be mild and no big deal, or you could be one of those who has lasting effects..."
You present this as if they're more or less equally probable alternatives. And of course they are not.
It's more appropriate to say they could get the virus and either be asymptomatic (which it seems every single positively tested college player has been so far?) and not be sick at all, or they could be sick and have flu like symptoms which they have a 99.XX% chance of recovering fully from, based on their age group. And this risk is equal to or less than the seasonal flu, for which they nor families took extraordinary precautions for in their entire lives. Yes they may transmit it to others - they must stay away from the elderly and those with preexisting conditions, as all in society must. In terms of long term effects, no one in the world has that answer. There have been several studies conducted, but even the authors of those studies are not drawing any certain or likely conclusions from them.
If society has said going back to campus is worth the risks, given the probabilities above, the only question is how much more risk are these players to be at, vs. a typical university student? They should have studied that and given them answer.
Ask Eduardo Rodriguez if the risk was worth it, now that he's dealing with Covid-related heart issues.
I don't know who that person is, but I don't rely on sample sizes of 1 for decision making, because that's not science. I assume this is someone who has heart issues that have been judged permanent by covd? This does happen with other pathogens, but it is excessively rare. Meanwhile I can cite the names of hundreds of thousands who've recovered with no issues at all. One is *a*** *****, my neighbor next door, she had it and is totally fine. Was nothing for her. Is that strong evidence that players will be fine? Of course not, it's only 1 person. That's why probabilities matter.
Since we’re talking about potential long term impacts, it may be a bit premature to say that your neighbor is fine.
https://elemental.medium.com/even-if-youre-asymptomatic-the-coronavirus-can-do-damage-4ab22451161a
Topol’s is not the only study that has identified these underlying lung issues. A report on asymptomatic Covid-19 patients, published June 18 in the journal Nature Medicine, found GGOs and other lung irregularities in 67% of the roughly three dozen people it examined.
How big a deal is this? No one’s sure.
“Ground-glass opacities are very common — we see it all the time and there are many things that can cause it,” says Adam Bernheim, MD, a cardiothoracic radiologist at Mount Sinai Hospital in New York City. But while GGO’s are common, the ones that are turning up among Covid-19 patients are distinctive. “If we see this very round shape and peripheral distribution, that’s atypical of other types of infections but it’s something we frequently see with [Covid-19],” he explains.
Bernheim has published work on GGOs and other lung effects associated with the novel coronavirus. He says that the presence of these abnormalities among asymptomatic patients is now well established, but the long-term consequences of these lung issues are not fully known. “We’ve seen patients with mild GGOs that heal completely, whereas others develop scar tissue almost like a skin injury, which is permanent,” he says. This scar tissue could cause or contribute to poor lung function and shortness of breath, or even, theoretically, a slight increased in the risk for lung cancer later in life.
If you are 18-22, you have a long life ahead of you, so the potential long term effects might be a little worrying. If you have ambitions of making millions as a professional athlete, those long term effects may be even more troubling. While there is a great deal that is unknown, it seems that the more we find out, the more likely it seems that at least some people may have long term impacts. Unfortunately that won’t be knowable until it is too late to take precautions.
if you are going to college and choose not to go to parties and you are not living in the dorms, you actually have a fair amount of control over your own personal risk. Football players are being required to have much more exposure than the typical student, spending hours at required practices, often in close proximity to others breathing heavily. They are also being required to travel. I think they have a legitimate argument that their required exposure is significantly higher than the typical college student. At least the ones with pro potential also have significantly more to lose if there does turn out to be long term lung or heart damage in less severe cases.
"While there is a great deal that is unknown, it seems that the more we find out, the more likely it seems that at least some people may have long term impacts."
This is absolutely not true, and not in any way grounded in science.
The rest of your post makes subjective arguments that college players are more at risk for catching covd than typical students. I could provide counterarguments I suppose, but don't need to: neither of us have studied this, so we don't know, but can agree that colleges should provide this answer to athletes.
“This is absolutely not true, and not in any way grounded in science.’
Since scientific studies are finding more and more indicators of potential concern, I’m not sure what the evidence for your statement is. Obviously we won’t have good science on long term impacts, but if studies wee not finding potential indicators of impacts in multiple organs it would be reasonable to say, early indications are that there are not likely to be long term impacts. When there are in fact a number of such studies, it seems fair to say that the opposite is true. There is more reason for concern that there may be long term impacts.
My girlfriend's brother is a professional lacrosse player who had COVID a month or so ago. They just started their (truncated) season a couple weeks ago, and a few days before their first game, the team physician determined that due to COVID he had a heart condition which made it unsafe for him to play. So as a pro athlete he's missing his season and has a heart condition that may impact him for the rest of his life. He's in his early 20s, his name is Jules Heningberg and he went to Rutgers if you'd like to look this up to confirm.
So yes, he had COVID, recovered fully and was healthy enough to prepare for the season but his lingering heart condition (which was not there pre-COVID) is impacting his ability to play and earn money as an athlete. I don't know that this is a risk a lot of these guys will want to make.
The alternatives do not have to be equally likely for us to take serious consideration of the possible lasting effects.
The current best data on the death rate from COVID-19 in Michigan for those aged 0-30 is 0.5%. That's low compared to other age groups. But it's still two orders of magnitude larger than the death rate from flu for college-aged individuals. Even if you're young, COVID is far more serious than the flu: the risks are NOT equal, and we should stop making that comparison. (EDIT: we have to be careful whether we mean likelihood of death given infection, vs likelihood of death per capita. Hard numbers are posted by dc and bodog below.)
(You can argue that Michigan, having been hit early, underrepresents the number of asymptomatic cases in computing that 0.5% because at first we were only testing people who were already symptomatic. Ok fine, but how many asymptomatic flu carriers are there each year? How many of them get tested? That group is probably even less properly counted. So the comparison stands (and I think this holds up even after edit, though we have to be careful whether we're comparing deaths per infection vs deaths per capita)
Now, there does seem to be some evidence that that 0.5% is made up almost entirely of people with what we generically keep calling "pre-existing conditions" (whether they knew it or not). But even in the college-aged population, there are people who do in fact have these pre-existing conditions. That's true even in the football-playing population, as Mo Hurst recently reminded us (and remember that even with the support of the Michigan Medical establishment available, his condition was not caught until the NFL combine!).
I just hope that in the end, all the players and their families are put in positions to be able to make un-pressured decisions as to what level of risk they want to accept for themselves. That's not a decision that "society" as a whole should be making, because "society" is not playing football.
These are human beings, not statistics, and it's completely understandable that they might not want to take the risk. My kid's going back to college and I'm worried as hell, but we let him (he's 20) make the decision. He's in great physical condition, an athlete, but we would be foolish to think that there isn't a risk. As we've seen in non-Covid times, young people discover they have underlying conditions accidentally. It's uncommon but it does happen. As a parent, you think of all these things because staying home could ameliorate these risks. It's a tough decision.
So you've relied on probabilities to determine the risk is low enough to allow him back to school. That is an informed decision.
It's completely fine to look at the probabilities and say no, I'm not going to play (or go back to school, or go back to work, etc) based on this. I don't care if the % likelihood is very small, because my decision is any level of risk is too great (or even the very low level of risk is too great). Everyone makes their decision for themselves and their families however they need to, and we must all respect those decisions. I certainly will and do.
My issue with your post is that it said "could be that this happens, could be that that happens, you don't know". That's not correct. There is a very high percentage probability that the not-bad thing happens, and a very low percentage that the bad thing happens. Given that knowledge, we all make decisions that fit us.
My initial post was purely about risk, but you glossed over that. I wrote, "If you play, you risk getting sick." That is accurate. I also said if you don't play, you risk losing a spot on the team next year because someone else may take your place, a new guy comes in or you lose training or playing experience. This is accurate. It's a risk either way. You seemed to home in on the way I characterized how the disease may manifest itself, but my post was about risk aversion, and having to pick between two different risks.
I didn't have any reason to dispute these other points, none of which were invalid.
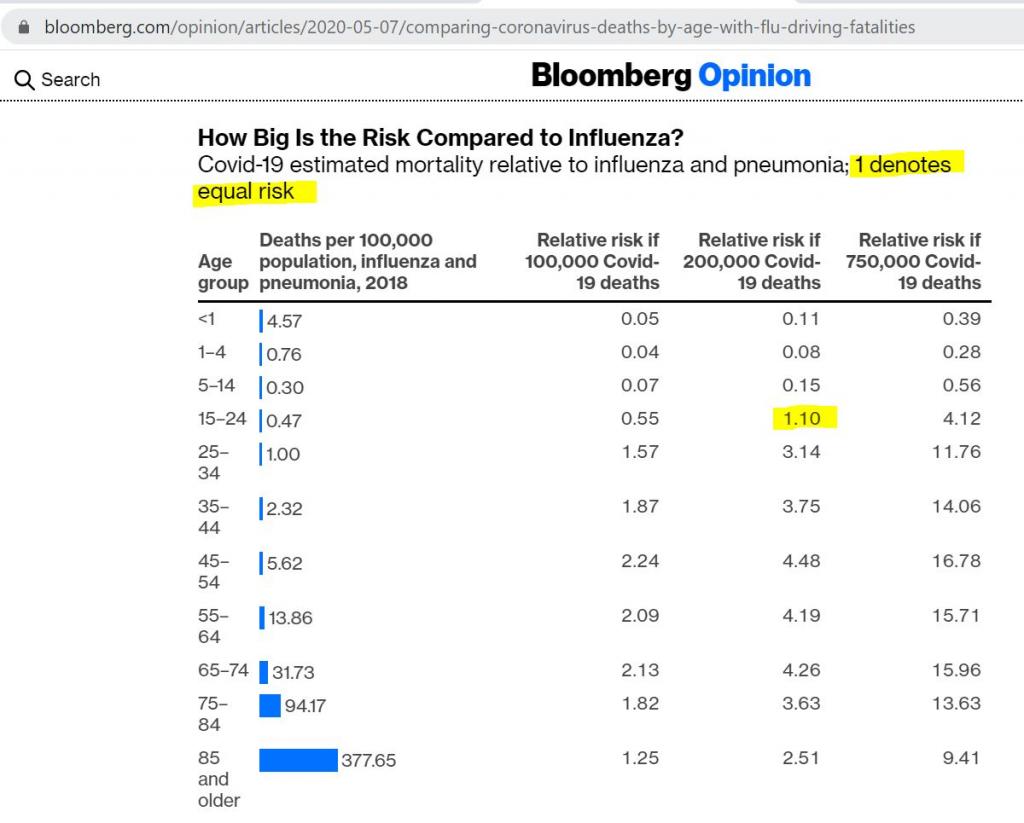
If you are talking purely mortality, based on this comparison done by Bloomberg, it is likely that there will be more deaths in the age group of 18-24 then in a relatively bad recent flu year (2018). This will occur at a bit less than 200,000 total deaths. While it is likely to ultimately be higher, it seems unlikely that it would be two orders of magnitude higher. We’d need over 350,000 US deaths for it to be twice as high.
https://www.bloomberg.com/opinion/articles/2020-05-07/comparing-coronavirus-deaths-by-age-with-flu-driving-fatalities However it is important to remember that the risk of death from flu for that age group is quite low. People in that age group are much more likely to die from a car accident than from either the flu or covid.
I don’t think the primary risk that people that age should be worried about is mortality, it is how much we don’t know about long term health risks. Some of the potential long term impacts like heart and lung damage might be particularly concerning to an elite athlete.
Thank you, I posted this very analysis a while back on this site, as evidence that college players are not at more risk from COVD than seasonal flu. At 200K deaths, it's roughly equal to seasonal flu (I will need to update my assumption from "less than or equal to" to "equal to", given the number of projected deaths has moved from what was 100K then to 200K now).
The studies done to date on long term effects are very limited and not at all ready to have conclusions be drawn from them.
Thank you; that was an interesting read. Note though that the author here is comparing flu deaths per capita to expected COVID deaths per capita, making three different assumptions about how many people will be infected with COVID. While these assumptions may provide reasonable bounds and therefore are more informative about how many people probably WILL die, they do not directly address the probability of death given infection, which is the number I argue is higher for COVID than for flu in my post above.
CDC estimates death rate per flu by (1) looking at death rate per hospitalization, (2) using previous data on hospitalizations per known infection. There does not appear to be any accounting for non-infectious carriers. Rather, they figure out what fraction of people go to the hospital for the flu by surveying people to find out how many with flu-like symptoms went to the hospital. See here:
https://www.cdc.gov/flu/about/burden/how-cdc-estimates.htm
In other words, like Michigan in March but unlike the USA in general right now, in a typical flu year we have no idea how many people got flu but were asymptomatic. We just know how many people reported symptoms.
The worst case assumption in the Bloomberg article about number of expected exposures is based on total deaths in NYC to date, which builds in all the social distancing, mask wearing, quarantining, etc that NYC has done -- admittedly a week or more too late, but real attempts have been made to curtail spread. Compare that to what we do in a typical bad flu year -- which, let's be honest, is pretty much nothing. What fraction of people in NYC do we think have actually been exposed to COVID? And even in that "worst" case, the author shows that COVID becomes an order of magnitude more deadly for a 15-24 year old than a bad flu would be. But again, you have to further scale that for what fraction of NYC you think has actually been exposed to COVID, vs the fraction that would be exposed to flu in a given year. We don't know either number, but given the extraordinary measures taken this year and the almost zero measures taken any other year, I think it's safe to say that far more people are exposed to flu in a normal year than to COVID this year.
So my point stands. Let's continue to socially distance, wash hands, wear masks, limit gatherings, whatever it takes to keep the number exposed in the US to the bottom end of the estimates. If we do that, then the number of young people who die of COVID likely will be comparable or smaller than what we'd see from a bad flu. And we should be strongly motivated to continue to take these steps, not just for the 40+ population, but because the intrinsic fatality rate per exposure for COVID is clearly at least an order of magnitude worse even at age 15, and probably younger still.
"then the number of young people who die of COVID likely will be comparable or smaller than what we'd see from a bad flu."
I agree for those aged 15-24, the COVD death rates are likely to be comparable to seasonal flu. For those 15 and younger, it is much, much less than that.
Your analysis is interesting but I will defer to the Bloomberg piece.
Because of both the way the data is generated and the way it is bracketed by age one can’t do an apples to apples comparison, but I think these numbers pretty clearly demonstrate that Covid is not an order of magnitude more deadly for younger people.
During the 2018/219 flu season, CDC estimated that there were 477 deaths for those aged 0 to 17. That was not a particularly bad flu year with about 34,000 deaths. https://www.cdc.gov/flu/about/burden/2018-2019.html
Through June 17, when there had been 103,000 deaths in the US. 26 were for children under the age of 14 and 151 were for those under the age of 25.
In other words, three times as many people under the age of 17 died from the flu as people under the age of 25 died from covid when we had about 100,000 covid deaths. It is hard to look at those numbers and believe that Covid is an order of magnitude worse for those under 15 if your measuring stick for worse is mortality.
August 2nd, 2020 at 10:18 AM ^
I agree that an apples-to-apples comparison is impossible from the data presented. This is precisely what I see as the problem with the Bloomberg article -- it comes across as an apples-to-apples comparison when it is not any such thing.
But I also think you and I are talking past each other. Your response appears to provide the answer to the question "given that 100,000 people have died total, what fraction of them are kids." You then show that this fraction is smaller for COVID than for a typical flu. This is a statement about the functional relationship between age and mortality rate for each disease, and a comparison of the two. I accept that relationship as demonstrated, and find it quite interesting.
My point is this is the wrong comparison to make, because like the Bloomberg article, it starts with "given that 100,000 people have died." That given includes an assumption about how many people have been exposed. But due to the extraordinary measures that have been taken this year (and the still-growing positive test count) it is clear that not everyone has been exposed. By contrast, in any other year, we do very little to limit our exposure to seasonal flu. Let's consider a counterfactual in which no social distancing, economic shutdown, etc etc were done this year and COVID were simply allowed to spread the way flu would in a typical year. How many deaths would this lead to for kids aged, say, 0-17? Not per 100,000, but total?
The worst case scenario in the Bloomberg article assumes for the entire US a mortality rate equal to that in NYC. But what fraction of people in NYC have actually been exposed? The Johns Hopkins dashboard currently lists 225,000 confirmed cases for a city of 8 million people. The exposure rate is unknown. We know testing didn't catch every case. Suppose the true number of infections is fully 3 times larger, or about 10% of the population of the city. Now suppose that no measures had been taken to limit spread. What fraction of that population would eventually have been exposed? This is hard to say for sure since it seems like a few "super-spreaders" (either individuals or events) are responsible for so much of the growth. Our best controlled experiment remains the Princess Diamond, where 19% of the passengers had symptoms, which given the rate of asymptomatic cases we see in places like North Carolina now, suggests that essentially 100% of the passengers were exposed. Now NYC is not a cruise ship, so let's cut that number in half and say a baseline non-quarantine exposure rate would be 50%. That means we'd take the Bloomberg article "worst case" scenario and multiply by another factor of 5. Scaled to the US, that's 3.75 million deaths; looking at 26 deaths per 100,000 gives you 975 deaths for ages 0-17. (That's also 3.75 million dead Americans, which, WOW.)
In other words, even for kids, COVID is at least as deadly as flu on a per-kid-exposed basis (not on a per-100,000-total-deaths basis). I cede that it is not two orders of magnitude as deadly. But it is only less fatal if you assume not every kid is exposed. Right now, that is true. Whether it stays this way if kids go back to school in person in the Fall remains to be seen.
Now to the larger picture, if COVID is comparable to but not worse than the flu for 0-17 year olds, that's wonderful, reassuring news. For the rest of us...
I would agree that the studies are limited and not at all ready to draw conclusions from them. You however seem quite comfortable drawing from this limited impact the fact that the risk is low, I’m at a loss as to how you draw that conclusion. Absence of knowledge is not the same thing as knowledge of absence.
"You however seem quite comfortable drawing from this limited impact the fact that the risk is low, I’m at a loss as to how you draw that conclusion."
I'm not at a loss. For whatever personal reason he's pretty clearly in the "Open her up!" crowd. His posts are mostly reasonable but they skew in a certain direction.
This would be the same as me labeling you and those above as being in the "we're all going to die!" crowd. This is a juvenile reaction.
Thank you for saying my posts are reasonable. I believe my view is informed by the science, and to the extent that you believe my posts skew in the direction of opening up the economy, it's because you see the science as pointed that way.
August 1st, 2020 at 10:19 PM ^
All it means is that your interpretation of the science points in a certain way. Whether the science actually points in that direction is a subject of reasonable debate.
August 1st, 2020 at 10:38 PM ^
Not if I'm not interpreting the data. At one extreme I could be posting actual scientific studies, and my counterpart could be posting 4chan conspiracy theories. In this scenario there is no interpretation, there is only science vs. non-science. You would be very incorrect if you said it was debatable whether actual science pointed in the direction my posts.
But of course we are all human beings with bias. It's not any more correct to say I'm in the "open 'er up" camp than to say these others are in the "we're all going to die!" camp.
August 1st, 2020 at 10:57 PM ^
Since most of your posts that use the word science don’t in fact even cite a scientific study, much less just post the scientific conclusion, I think your own argument makes my point - at best you are interpreting the data.
August 1st, 2020 at 10:30 PM ^
You make good arguments. I need to take a deeper look at some of these studies. However, I stand by my conclusion that none of them have provided sufficient information upon which to make judgments. They are too early, too small, too inconclusive, and even the researchers themselves generally assert that. Given that, my view is the "but what about the possible long term effects" concerns now pervading the national discourse are very premature.
Three things based on this. First, if the studies prove to be true - or are even of enough concern to be considered in decisions like college football - then this is an argument to shut down the economy until there's a vaccine. Forget about football. I don't see many people anywhere in the world advocating for this. There would be much more energy around that if the studies were enough to be truly concerned. Second, it seems like the goalposts keep moving: first it was millions will die, then it was flatten the curve, now that those have been debunked and accomplished, and it's been established that young people are at minimal risk, there is now this amorphous "but what about the possible long term effects" argument. I want to see this as an established, real risk before I personally make decisions based upon it. And I'd like to see the country do the same. Finally, I believe "but what about the long term risks will eventually fade to the background very similarly to the Kawasaki syndrome concerns raised months ago. This is admittedly a gut feel, but it feels very similar.
August 1st, 2020 at 11:17 PM ^
Since we are on a sports forum, in a post talking about football it seems entirely rational to focus on football. That is the question at hand. To the extent that many of the potential long term effects being contemplated are in fact cardiovascular, it is not hard to understand why someone with professional athletic aspirations might be particularly concerned. Small differences in performance can make a big difference in both your ability to make a professional team and your potential salary.
With regards to moving the goalpost, I’d argue that the goalpost has always been keep hospitals from getting overwhelmed. Since that continues to be a reoccurring challenge, I don’t think the goalposts have been moved. Obviously whether hospitals have been or would have been absent extreme measures is a subject for debate, I’ll give you my personal definition. If you need to cancel elective surgeries for any significant amount of time, you’ve reached a point where you are flirting with overwhelming your hospital. If you need to keep patients in the ER for much longer times than usual because you do not have ICU space available, you are flirting with overwhelming your hospitals. If you are turning away ambulances at much greater rates than normal, you are flirting with overwhelming your hospitals. This has happened in multiple states (including a number in July) since Covid started. If you are insistent, I can find you documentation (I’ve already done it Many times on this board).
Finally, with regards to long term risks, is it really surprising that less than 5 months into what is one of the greatest health crisis this country has faced since the Spanish Flu we are only beginning to see science on long term effects? Hopefully you are right and it will be a minor issue, unfortunately hope is not science.
I believe nearly anyone in the scientific community would agree that the current death rate you note is certain to be overstated once the final data is established. See below from another poster for a better analysis from Bloomberg.
My use of the term "society" was in regard to the decision to return students to campus, not about players playing football. That was clear, but if you didn't understand my point, I was saying that universities have already judged (by and large) that returning to students to campus is worth the risk*; assuming these athletes will then be returning to school, the only difference is how much more or less risk they incur by being football players. Then the decision can be made based on that.
*Of course any parent or student can disagree with this and opt to stay out of school, based on their gauge of the risks
I did understand your point, but appreciate the clarification. What I find significant in the context of the originally posted article is the same point you just made: universities have decided that the risk is tolerable, but individual students may disagree. Which is fine, people are free to make whatever decision makes sense for them and their situation. I wonder whether the scholarship college athlete faces the same degree of freedom in opting in or out of playing this year when the powers that be (Sankey & co in the case of the OP) decide the risk is worth it to them.
August 1st, 2020 at 10:05 PM ^
Yes of course they do. It was announced two weeks ago that the SEC would honor scholarships for athletes opting out (as did the B1G, Pac12 and ACC). Everyone expected this, and it's come to pass. I thought this was common knowledge and is of course part of my statement: athletes will go to school because the universities are going back, so the only thing to understand is whether they have higher or lower risk if they're going to play vs. being a normal student. And as I've said, the university should have studied this, and this should really be the central question around which the decisions are made. Of course yes, the individual student has the choice not to return to school. This is true of its corollary as well, but since these things seem to be being missed in this conversation and I'm here anyway: if an athlete is choosing not to go back to school, then of course he is not going to play football; this is obviously also his right and everyone will respect his decision.
August 1st, 2020 at 10:43 PM ^
In many schools that are going back, “normal” students have the option of taking their classes fully online. A number of prominent football schools have at a minimum announced delays in on campus instruction (Students at Clemson start class on August 19, but move in day is not until September 13 and in person instruction does not begin until September 21. UCLA is primarily on-line. In the big 10, Illinois, Maryland and Minnesota are all primarily online.
https://www.chronicle.com/article/heres-a-list-of-colleges-plans-for-reopening-in-the-fall/
So obviously it is not universally true that athletes will go back to school because the Universities are going back.
College Player: “What information do you have about the lasting effects on players who may contract COVID?”
SEC Commissioner Stankey: “Although I bank 2.5 million to lead this conference I came unprepared to respond to reasonable questions..... therefore, I’ll pass the buck to...um...Shawn....take a swing...”
Shawn Gibbs, Dean TAMU School Public Health: “Don’t look at me, I’m an industrial hygienist..... I’m no medical person....”
College Player: “All due respect Shawn but why the hell are you on this call?
Shawn: “...so I don’t get fined...“
Once again proving the right collection of college aged people can be far more insightful, thoughtful, and reasonable than then wrong collection of older adults.
It's an interesting article, and while I don't believe it's safe yet to have a football season I do completely understand why people (including athletes and staff) want to give it a go. I truly do. But I think the athletes bring up some really solid points and the SEC officials, well, sort of hand-wave them a bit away with "nobody can give you 100% certainty" responses.
I do think this paragraph embodies why I am (and I assume others are) really bothered by the various athletic department officials pushing so hard to open the season despite a lot of evidence that we as a country aren't really set up to handle it.
Sankey, who earned a $2.5 million salary in 2018, responded: “Part of our work is to bring as much certainty in the midst of this really strange time as we can so you can play football in the most healthy way possible, with the understanding there aren’t any guarantees in life."
That's a man with a guaranteed contract worth millions telling a bunch of unpaid college athletes they gotta take some risks in life. And yet, I recognize that there are thousands of staff and school employees who may well lose their jobs if sports aren't played in the fall. But that responsibility shouldn't be placed on the shoulders of college students receiving, at best, tepid assurances from school leaders about what dangers are posed to them.
Yeah, that was nicely juxtaposed by the writer.